
By Ali Weatherford
I honestly didn’t know what my cervix was while I was pregnant and giving birth. Maybe that was covered in 6th grade health class, but I was not paying attention!
During my pregnancy, I didn’t think to ask questions about my anatomy. I’m not sure why. I don’t remember, but I might have been a little embarrassed that I didn’t know what those things were. I might also have just wanted to ignore as much as possible.
Like many of you probably are, I was nervous about what was going to happen and not all that excited to find out. I didn’t know that it might be helpful to understand more about my anatomy for pregnancy and birth.
Now that I’m a childbirth educator, I’m pretty amazed at the human anatomy that makes pregnancy and birth possible. I love talking about those parts and how they work, and the uterus is my favorite organ. The cervix is a very important part of the uterus.
What is the cervix exactly?
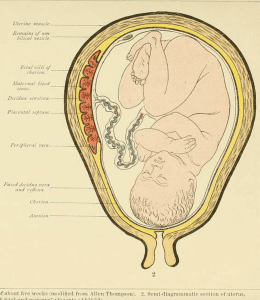
You can see the uterus in this drawing on the left. The part at the bottom that looks like a neck, or two thumbs pointing down, is the cervix. You can see in the picture that the color of the cervix is a little different from the rest of the uterus. There is no shading in the image. That’s because while most of the uterus is made of very strong muscle fiber, the cervix is not. The cervix is a little bit muscular but mostly connective tissue, so it behaves differently from the rest of the uterus.
What does the cervix do?
During pregnancy, the cervix stays long and firm and tightly shut and sealed. This ensures that your baby doesn’t come out too soon, and that nothing else can get in. As you are nearing the end of pregnancy, there will be some changes.
- Ripening: The cervix will soften in response to some hormonal changes. A very unripe cervix might feel like the tip of your nose. A very ripe cervix will feel more like your ear lobe.
- Effacement: As it softens, the cervix will begin to thin out and pull back from the opening. Effacement is measured as a percentage. 10% effacement feels like the cervix is that much shorter. 100% effacement means the cervix is completely thinned out and feels very short or on level with the rest of the uterus.
- Dilation: The cervix will open. As it’s opening, it might be compared to what it looks like when a closed eye opens gradually. Dilation is measured in centimeters. Fully closed would be 0cm, and fully open is 10cm. I just measured it, and that’s exactly the length of the mouse I’m using to write this article right now!
Some of these changes can start before labor, and sometimes they all happen during labor. Sometimes the changes are gradual and slow, but once the uterus is contracting strongly, the cervix might change very dramatically and very quickly.
It will get very soft. It will shorten until it barely sticks out at all. And it will open until it’s completely dilated. Once all of those changes are made, a baby can get through.
You’ll probably be asked to allow cervical exams during prenatal visits, and also to monitor the progress during labor.
How is a cervical check done?
A nurse, doctor, or midwife will insert two gloved fingers into the vagina and feel the cervix. They do not use a ruler or special measuring tool to assess the cervix. Some people have big hands, some have small hands. They have to estimate. This means it’s pretty subjective, and there is room for error. During a cervical check, one person might feel 80% effacement and 5cm of dilation, but another might say 70% and 4cm. So who do you believe? I think it’s safe to say you can believe whatever makes you happy!
Before any of that happens though, it’s important that you are informed about the procedure and that you give consent. In the best situations, you would hear all of these things:
- I would like to do a cervical check because……
- I’ll need you to get into this position…..
- Here’s what it might feel like……
- Here’s how long it will take……
- Here’s why I think it will benefit you…….
- These are some risks of doing this assessment……
- How do you feel about that? Do you want to go ahead?
Once you have all of the information, you can choose whether or not to go through with the cervical check. You have the right to give consent to or to refuse the procedure. You should ALWAYS be asked for your permission first.
It’s true that sometimes cervical checks happen without permission. It’s unfortunate, but sometimes it’s assumed that once you’re in the hospital or birth center, anything is allowed. That is not the case. Just being a patient doesn’t mean that things should be done without explanation and approval.
Also, hospitals can be very busy places. Sometimes care providers are overworked and hospitals are overcrowded. Unfortunately, this can create a stressful situation for the staff which sometimes means they have to move too quickly and might overlook things, even when they have very good intentions. Most of the time, checking without permission is an accidental oversight.
For a lot of people, it’s also helpful to get some narration during the procedure. “Okay, now you can let your knees relax open. I’ll insert 2 fingers now. It might feel a little cold. You might be feeling a little pressure. I can feel the cervix now. It feels very soft. It looks like you’re fully effaced and about 6 cm dilated. I’m all finished now.” It can be comforting to know exactly what will happen, and what is going on WHILE it’s happening too. It’s very reasonable to ask for that.
Do I need a lot of cervical checks?
The standard in hospitals used to be to perform a cervical check almost every hour. Evidence does not support this practice. Checking that often is not shown to improve outcomes.
Now the standard is to check less often, but it’s also good to know that most of them are optional. A cervical exam can really just tell you one thing, how your cervix looks RIGHT NOW. It can not predict what will happen next. If your cervix is fully dilated, it does not necessarily mean you’re ready to push and that your baby will be born in the next hour. If your cervix is not dilating much at all, it doesn’t mean that you won’t be giving birth in the next hour.
It’s true that it can help make better guesses, but that might actually make things harder for some people. It might be discouraging to find out that you’ve been laboring for 12 hours and that you’re “only” 3cm dilated. You might start to wonder if it’s really going to take four hours per centimeter! If that math is true, it would mean another 36 hours of labor. That would be very hard to hear.
Fortunately, that’s just not the way labor tends to work. For most people, the first 5cm take the longest. After that, dilation might happen at a MUCH faster rate. As your labor moves along, the contractions get longer, stronger, and closer together. Each contraction is doing something to make your cervix ready, so that means more progress more quickly. So, if you think you might feel discouraged knowing about the progress of your cervix, you might consider choosing them wisely.
A lot of people ask me which cervical checks are the most necessary. This is a hard question to answer, because it really does depend on each person and each situation. It’s best to talk it over with your care provider if a situation comes up where you’re being asked to consent to a cervical check that you’re not sure you want. They’ll be able to tell you if there’s a good reason.
In general though, I can think of four situations where you might like the idea of getting checked, even if you generally don’t want the exams. These may also be situations where you would be more strongly encouraged to consent to a check by your care providers.
- Before admission to the hospital or birth center: When you show up at your birth place, they usually want to know if you’re having real productive labor. Sometimes people do show up in “false labor” or just way too soon to be admitted. Checking your cervix can help decide whether it would be a good idea to stay or whether you could benefit from going home. It can also help them know whether your doctor or midwife should be called quickly, or whether that can wait.
- Before pushing: In most cases, feeling an urge to push means your body is ready for you to push. It’s a mostly reliable way to guide your pushing and birth. But in some rare situations, a person will feel an urge to push when the cervix is not ready to let the baby out yet. If you start pushing before the cervix is open enough, it can cause swelling and make things more complicated and difficult. This is why a cervical check might be strongly recommended before you start pushing.
- Before getting an epidural or pain medication: If your goal was to avoid medication unless absolutely necessary, and then you reach a very intense point in your labor and want to ask for medication, it might be a good idea to ask for a cervical check first. Often, people feel the most intense contractions right before full dilation when it’s time to start pushing and give birth. If you get a cervical check and find out that you’re fully dilated or almost there, you might decide not to get the medication.Most people benefit from having medication most before it’s time for pushing. The pushing part is usually not when people most need the pain relief. It can take at least 30-45 minutes for an epidural to provide relief, and by then you may not even need it anymore. Also, it’s pretty common for people to allow the medication to wear off during pushing so they can have a little more muscle control and ability to move.
- Before labor induction: If you schedule a labor induction, a cervical check is usually part of this process. There are many different methods that can be used to induce labor, and it can help your provider decide on the best course of action to know how ready your cervix is. They’ll need to do a cervical exam to find out.
Why not get cervical checks?
You may be perfectly happy getting many cervical checks. For some people they are not all that uncomfortable. Some people really like hearing about changes in the cervix, and it gives them some level of comfort.
On the other hand, you might feel very different. Sometimes checks are very uncomfortable or even painful. For most people, they’re at least a little bit uncomfortable. And some people have conditions that make any kind of penetration excruciating. If you’re in labor, it’s usually a good idea to get them in-between contractions instead of during a contraction to help with the physical discomfort.
For some people, they can also be emotionally painful. If you have experienced sexual abuse or trauma, a cervical exam might be extremely disturbing.
If you have any of these concerns, and want to limit cervical checks, that is absolutely reasonable. You can talk to your care team about which checks are most valuable or necessary before you decide whether or not to give consent. You can definitely share your concerns and difficulties with your care team, but you can also keep that information to yourself. You never have to justify your refusal with reasons. It’s OK to just say “No, thank you.”